Medical Disclaimer: This is educational content only, not medical advice. Consult a licensed healthcare provider for diagnosis/treatment. Information based on sources like WHO/CDC guidelines (last reviewed: 2026-02-13).
This article is being expanded for more depth. Check back soon!
Electrocardiogram ECG Interpretation Guide for Medical and Clinical Practice
Frequently Asked Questions
What is an ECG?
An electrocardiogram (ECG) is a non-invasive test that records the electrical activity of the heart over time to assess heart rhythm, rate, conduction abnormalities, ischemia, and structural heart disease.
What does a normal ECG show?
A normal ECG shows sinus rhythm with a rate of 60–100 bpm, normal P waves before each QRS complex, PR interval 120–200 ms, QRS duration <120 ms, and no significant ST-T abnormalities.
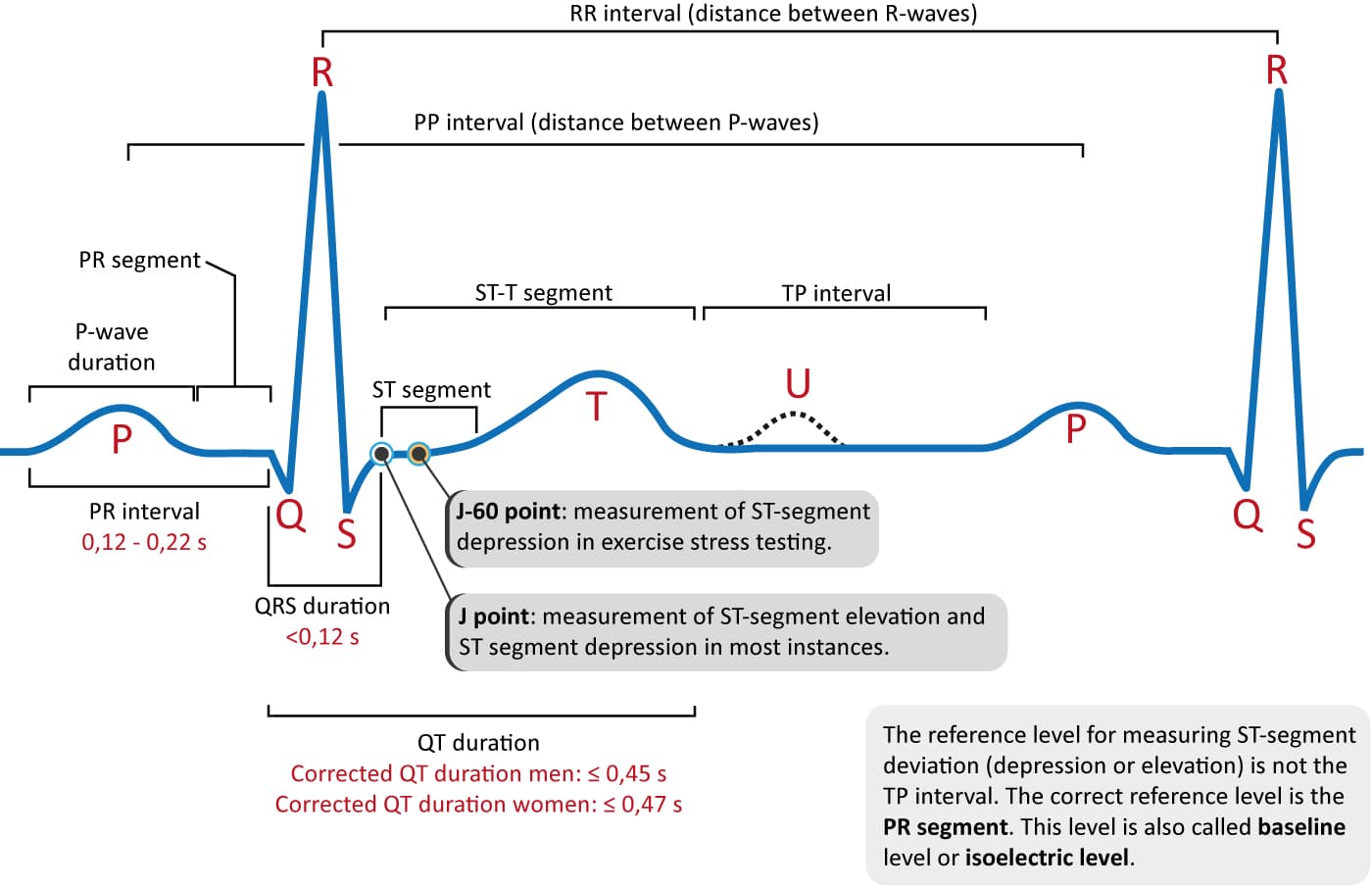
What are the main components of an ECG waveform?
The main components are the P wave (atrial depolarization), PR interval (AV conduction), QRS complex (ventricular depolarization), ST segment, T wave (ventricular repolarization), and QT interval.
How many leads are used in a standard ECG?
A standard ECG uses 12 leads: 6 limb leads (I, II, III, aVR, aVL, aVF) and 6 precordial chest leads (V1–V6).
What does ST elevation on ECG indicate?
ST elevation usually indicates acute myocardial injury, most commonly ST-elevation myocardial infarction (STEMI), but can also be seen in pericarditis, early repolarization, and ventricular aneurysm.
What ECG changes are seen in myocardial infarction?
Typical changes include hyperacute T waves, ST elevation or depression, pathological Q waves, and T wave inversion depending on the stage and location of infarction.
What is the significance of QT interval prolongation?
Prolonged QT interval increases the risk of torsades de pointes, a potentially life-threatening polymorphic ventricular tachycardia.
How is heart rate calculated on ECG?
In regular rhythm, heart rate is calculated as 300 divided by the number of large squares between two R waves. In irregular rhythm, QRS complexes are counted in 10 seconds and multiplied by 6.
What ECG findings suggest atrial fibrillation?
Atrial fibrillation shows an irregularly irregular rhythm with absent P waves and variable R–R intervals.
What is a wide QRS complex and what does it indicate?
A wide QRS complex (>120 ms) suggests abnormal ventricular conduction such as bundle branch block, ventricular rhythm, hyperkalemia, or drug toxicity.
What are common ECG changes in electrolyte abnormalities?
Hyperkalemia causes tall peaked T waves and wide QRS, hypokalemia causes U waves and flat T waves, hypercalcemia shortens QT interval, and hypocalcemia prolongs QT interval.
What is axis deviation on ECG?
Axis deviation refers to abnormal direction of ventricular depolarization. Left axis deviation and right axis deviation are associated with specific cardiac and pulmonary conditions.
What ECG features indicate pericarditis?
Acute pericarditis typically shows diffuse ST elevation with PR segment depression across multiple leads.
Can ECG be normal in heart disease?
Yes, ECG can be normal in early ischemia, stable angina, or some structural heart diseases, so clinical correlation is always required.
Why is ECG important in emergency medicine?
ECG provides rapid diagnosis of life-threatening conditions such as myocardial infarction, ventricular arrhythmias, heart block, and electrolyte disturbances, guiding immediate management.
MCQ Test - Electrocardiogram ECG Interpretation Guide for Medical and Clinical Practice
Progress:
0/15
Time: 00:00
Test Results
0%
0/15
0
Correct Answers
0
Wrong Answers
00:00
Time Taken
0
Skipped