Medical Disclaimer: This is educational content only, not medical advice. Consult a licensed healthcare provider for diagnosis/treatment. Information based on sources like WHO/CDC guidelines (last reviewed: 2026-02-13).
This article is being expanded for more depth. Check back soon!
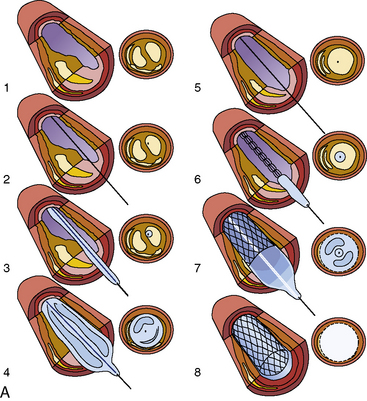
Percutaneous Coronary Intervention PCI Procedure Indications Risks And Management
Frequently Asked Questions
What is percutaneous coronary intervention (PCI)?
Percutaneous coronary intervention is a minimally invasive cardiac procedure used to open narrowed or blocked coronary arteries using a catheter-based approach, usually involving balloon angioplasty and stent placement to restore myocardial blood flow.
When is PCI most strongly indicated?
PCI is most strongly indicated in acute ST-elevation myocardial infarction (STEMI), high-risk non-ST elevation acute coronary syndromes, and in patients with refractory angina despite optimal medical therapy.
What is the difference between PCI and coronary angiography?
Coronary angiography is a diagnostic procedure used to visualize coronary arteries, whereas PCI is a therapeutic intervention performed to treat significant coronary artery stenosis identified during angiography.
What are drug-eluting stents (DES)?
Drug-eluting stents are coronary stents coated with antiproliferative drugs such as sirolimus or everolimus that reduce neointimal hyperplasia and significantly lower the risk of in-stent restenosis.
What is dual antiplatelet therapy after PCI?
Dual antiplatelet therapy consists of aspirin plus a P2Y12 inhibitor such as clopidogrel, ticagrelor, or prasugrel, used to prevent stent thrombosis following PCI.
How long is dual antiplatelet therapy required after PCI?
After drug-eluting stent implantation, DAPT is recommended for at least 12 months in acute coronary syndrome and at least 6 months in stable coronary artery disease, unless bleeding risk dictates otherwise.
What are the common complications of PCI?
Common complications include bleeding at the access site, contrast-induced nephropathy, coronary artery dissection or perforation, acute stent thrombosis, arrhythmias, and in-stent restenosis.
Why is radial artery access preferred for PCI?
Radial artery access is preferred because it significantly reduces bleeding and vascular complications, allows early ambulation, and improves overall patient comfort compared to femoral access.
Does PCI improve survival in all patients with coronary artery disease?
PCI provides a clear survival benefit in acute coronary syndromes, especially STEMI, but in stable coronary artery disease it mainly improves symptoms and quality of life rather than long-term mortality.
What factors increase the risk of stent thrombosis?
Premature discontinuation of dual antiplatelet therapy, stent under-expansion, high thrombus burden, diabetes mellitus, renal failure, and complex coronary lesions significantly increase the risk of stent thrombosis.
MCQ Test - Percutaneous Coronary Intervention PCI Procedure Indications Risks And Management
Progress:
0/0
Time: 00:00
No MCQs available for this article.