Medical Disclaimer: This is educational content only, not medical advice. Consult a licensed healthcare provider for diagnosis/treatment. Information based on sources like WHO/CDC guidelines (last reviewed: 2026-02-13).
This article is being expanded for more depth. Check back soon!
Cushing Syndrome Comprehensive Clinical Guide Diagnosis Causes and Management
Frequently Asked Questions
What is Cushing syndrome?
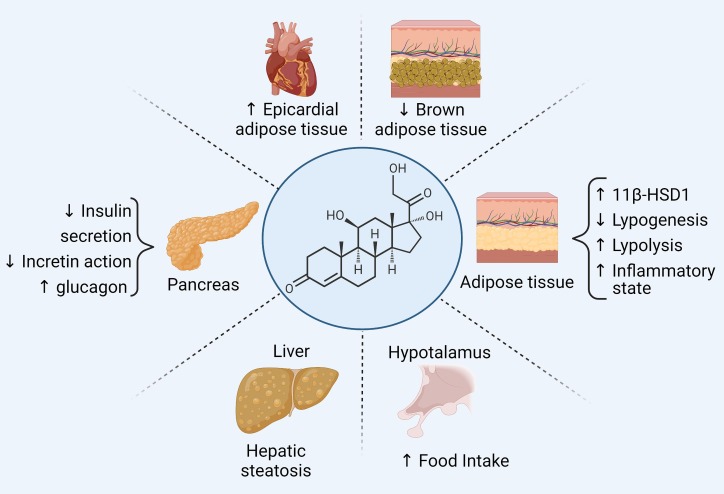
Cushing syndrome is a clinical condition caused by chronic exposure to excess glucocorticoids, either from exogenous steroid use or endogenous overproduction of cortisol.
What is the difference between Cushing syndrome and Cushing disease?
Cushing syndrome refers to all causes of cortisol excess, while Cushing disease specifically refers to cortisol excess due to an ACTH-secreting pituitary adenoma.
What is the most common cause of Cushing syndrome?
The most common cause of Cushing syndrome is exogenous glucocorticoid therapy.
What are the classic clinical features of Cushing syndrome?
Classic features include central obesity, moon face, buffalo hump, purple striae, proximal muscle weakness, hypertension, diabetes, osteoporosis, and easy bruising.
How is Cushing syndrome initially screened?
Initial screening includes overnight 1 mg dexamethasone suppression test, 24-hour urinary free cortisol, or late-night salivary cortisol measurement.
Why is late-night salivary cortisol important in diagnosis?
It detects loss of normal diurnal cortisol rhythm, which is a hallmark of Cushing syndrome.
How is ACTH-dependent Cushing syndrome differentiated from ACTH-independent causes?
Plasma ACTH levels are measured; low ACTH suggests ACTH-independent causes, while normal or high ACTH indicates ACTH-dependent Cushing syndrome.
What causes hypokalemia in ectopic ACTH syndrome?
Very high cortisol levels activate mineralocorticoid receptors, leading to potassium loss and metabolic alkalosis.
What is the gold standard test to localize ACTH source?
Inferior petrosal sinus sampling is the gold standard for distinguishing pituitary from ectopic ACTH secretion.
What is the definitive treatment for Cushing disease?
Transsphenoidal surgical removal of the pituitary adenoma is the definitive treatment.
When is medical therapy used in Cushing syndrome?
Medical therapy is used when surgery is contraindicated, as a bridge to surgery, or in persistent or recurrent disease.
Which drugs reduce cortisol synthesis in Cushing syndrome?
Ketoconazole, metyrapone, and osilodrostat reduce cortisol synthesis by inhibiting adrenal steroidogenesis enzymes.
Why must steroids be tapered gradually in exogenous Cushing syndrome?
Gradual tapering prevents adrenal crisis due to hypothalamic-pituitary-adrenal axis suppression.
What are common complications of untreated Cushing syndrome?
Complications include cardiovascular disease, diabetes, osteoporosis, infections, psychiatric disorders, and increased mortality.
What is the most common cause of death in Cushing syndrome?
Cardiovascular disease is the leading cause of mortality in patients with Cushing syndrome.
MCQ Test - Cushing Syndrome Comprehensive Clinical Guide Diagnosis Causes and Management
Progress:
0/15
Time: 00:00
Test Results
0%
0/15
0
Correct Answers
0
Wrong Answers
00:00
Time Taken
0
Skipped