Medical Disclaimer: This is educational content only, not medical advice. Consult a licensed healthcare provider for diagnosis/treatment. Information based on sources like WHO/CDC guidelines (last reviewed: 2026-02-13).
Congenital Heart Disease Complete Guide Causes Types Diagnosis and Treatment
Frequently Asked Questions
What is congenital heart disease?
Congenital heart disease (CHD) refers to structural or functional abnormalities of the heart or great vessels that are present at birth due to abnormal cardiac development during embryogenesis.
How common is congenital heart disease?
Congenital heart disease occurs in approximately 8–10 per 1,000 live births, making it the most common congenital anomaly worldwide.
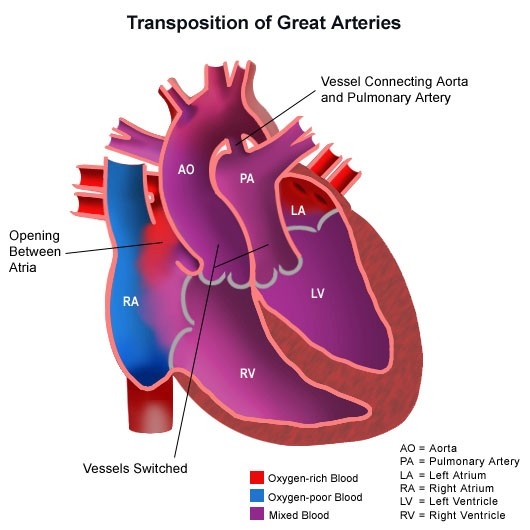
What are the main types of congenital heart disease?
CHD is broadly classified into acyanotic defects (such as ASD, VSD, PDA), cyanotic defects (such as Tetralogy of Fallot, Transposition of Great Arteries), obstructive lesions (coarctation of aorta, aortic stenosis), and complex congenital heart diseases.
What causes congenital heart disease?
Causes include genetic factors, chromosomal abnormalities, maternal diabetes, maternal infections like rubella, teratogenic drug exposure, alcohol use, and multifactorial environmental influences.
What are the common symptoms of congenital heart disease in newborns?
Common symptoms include cyanosis, rapid breathing, poor feeding, failure to thrive, excessive sweating, lethargy, and signs of heart failure or shock.
What is duct-dependent congenital heart disease?
Duct-dependent CHD refers to defects where systemic or pulmonary circulation depends on a patent ductus arteriosus for survival, requiring prostaglandin E1 infusion to maintain ductal patency.
How is congenital heart disease diagnosed?
Diagnosis is made using clinical examination, pulse oximetry screening, echocardiography, ECG, chest X-ray, and advanced imaging such as cardiac MRI or cardiac catheterization when required.
Can congenital heart disease be detected before birth?
Yes, many congenital heart defects can be detected prenatally using fetal echocardiography, usually performed during the second trimester.
What is Eisenmenger syndrome?
Eisenmenger syndrome is a late complication of uncorrected left-to-right shunt lesions where long-standing pulmonary hypertension leads to reversal of the shunt and development of cyanosis.
How is congenital heart disease treated?
Treatment depends on the defect and may include medical management, catheter-based interventions, or surgical correction, along with long-term follow-up and supportive care.
Is surgery always required for congenital heart disease?
No, small defects may close spontaneously or remain asymptomatic, while moderate to severe defects usually require interventional or surgical correction.
What medications are commonly used in congenital heart disease?
Common medications include prostaglandin E1, diuretics, ACE inhibitors, beta blockers, antiarrhythmics, and anticoagulants depending on the condition and complications.
What are the long-term complications of congenital heart disease?
Long-term complications may include heart failure, arrhythmias, pulmonary hypertension, infective endocarditis, exercise intolerance, and need for re-intervention.
Can adults live with congenital heart disease?
Yes, most children with CHD now survive into adulthood due to advances in medical and surgical care, but many require lifelong follow-up in adult congenital heart disease clinics.
Is infective endocarditis prophylaxis required in congenital heart disease?
Endocarditis prophylaxis is recommended only for high-risk conditions such as unrepaired cyanotic CHD, prosthetic valves, or previous infective endocarditis.
Can women with congenital heart disease become pregnant?
Many women with CHD can have successful pregnancies, but pregnancy requires careful risk assessment and management by a multidisciplinary cardiac and obstetric team.
How can congenital heart disease be prevented?
Prevention includes good antenatal care, control of maternal illnesses, avoidance of teratogenic drugs, vaccination against rubella, genetic counseling, and early screening.
What is the prognosis of congenital heart disease?
Prognosis varies widely depending on the type and severity of the defect; simple lesions often have excellent outcomes, while complex CHD requires lifelong care.
MCQ Test - Congenital Heart Disease Complete Guide Causes Types Diagnosis and Treatment
Progress:
0/15
Time: 00:00
Test Results
0%
0/15
0
Correct Answers
0
Wrong Answers
00:00
Time Taken
0
Skipped