Medical Disclaimer: This is educational content only, not medical advice. Consult a licensed healthcare provider for diagnosis/treatment. Information based on sources like WHO/CDC guidelines (last reviewed: 2026-02-13).
This article is being expanded for more depth. Check back soon!
Hypothyroidism Complete Guide Causes Symptoms Diagnosis and Treatment
Frequently Asked Questions
What is hypothyroidism?
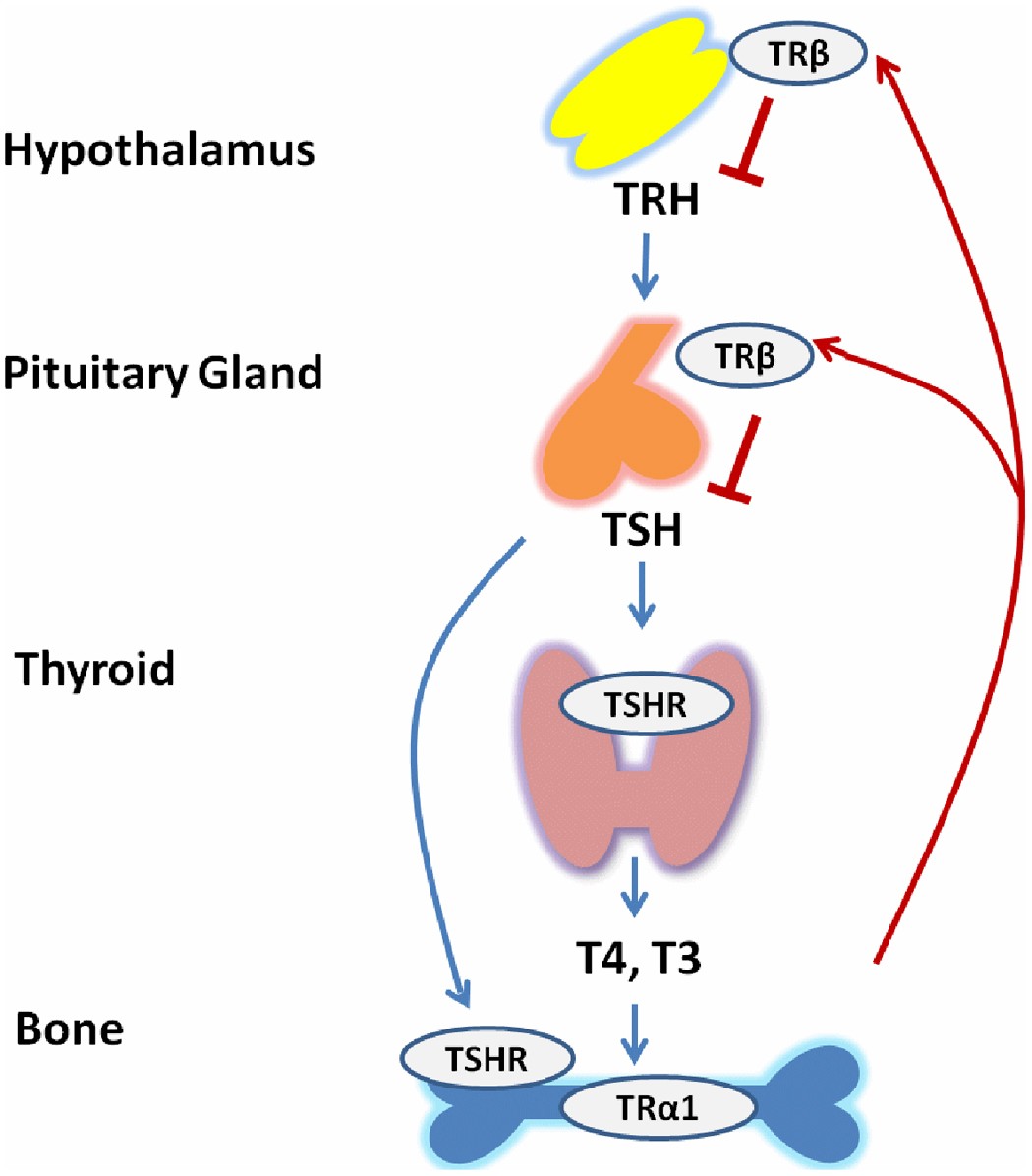
Hypothyroidism is a condition in which the thyroid gland produces insufficient amounts of thyroid hormones (T4 and T3), leading to a generalized slowing of metabolic processes in the body.
What is the most common cause of hypothyroidism?
The most common cause is Hashimoto thyroiditis, an autoimmune disorder in which antibodies destroy thyroid tissue.
What are the typical symptoms of hypothyroidism?
Common symptoms include fatigue, cold intolerance, weight gain, constipation, dry skin, hair loss, depression, bradycardia, and menstrual irregularities.
How is hypothyroidism diagnosed?
Diagnosis is primarily made by laboratory testing showing elevated TSH with low free T4 in primary hypothyroidism.
What is subclinical hypothyroidism?
Subclinical hypothyroidism is defined by elevated TSH levels with normal free T4 levels, often with mild or no symptoms.
When should subclinical hypothyroidism be treated?
Treatment is recommended when TSH is greater than 10 mIU/L, in symptomatic patients, during pregnancy, or when anti-TPO antibodies are positive.
What is the treatment of choice for hypothyroidism?
Levothyroxine (synthetic T4) is the treatment of choice and is usually required lifelong in primary hypothyroidism.
How should levothyroxine be taken?
Levothyroxine should be taken orally on an empty stomach, preferably in the morning, 30–60 minutes before food, and separated from calcium or iron supplements by at least 4 hours.
How is treatment monitored in hypothyroidism?
TSH levels are monitored every 6–8 weeks after starting or adjusting therapy, and once stable, every 6–12 months.
Why is TSH unreliable in secondary hypothyroidism?
In secondary hypothyroidism, pituitary dysfunction leads to inappropriately normal or low TSH, so free T4 is used for monitoring.
What complications can occur if hypothyroidism is untreated?
Complications include hyperlipidemia, cardiovascular disease, infertility, anemia, hyponatremia, and myxedema coma.
What is myxedema coma?
Myxedema coma is a life-threatening complication of severe hypothyroidism characterized by hypothermia, altered mental status, bradycardia, and respiratory failure.
Why are steroids given before thyroid hormone in myxedema coma?
Steroids are given to prevent precipitating adrenal crisis due to possible coexisting adrenal insufficiency.
Does hypothyroidism affect pregnancy?
Yes, untreated hypothyroidism increases the risk of miscarriage, preeclampsia, and impaired fetal neurodevelopment.
Is hypothyroidism a lifelong condition?
In most cases, especially autoimmune hypothyroidism, it is lifelong and requires continuous thyroid hormone replacement.
MCQ Test - Hypothyroidism Complete Guide Causes Symptoms Diagnosis and Treatment
Progress:
0/15
Time: 00:00
Test Results
0%
0/15
0
Correct Answers
0
Wrong Answers
00:00
Time Taken
0
Skipped