Medical Disclaimer: This is educational content only, not medical advice. Consult a licensed healthcare provider for diagnosis/treatment. Information based on sources like WHO/CDC guidelines (last reviewed: 2026-02-13).
This article is being expanded for more depth. Check back soon!
Differential Diagnosis of Jaundice Complete Causes Types Clinical Approach
Frequently Asked Questions
What is jaundice?
Jaundice is yellow discoloration of the skin, sclera, and mucous membranes caused by elevated serum bilirubin levels, usually above 2–3 mg/dL.
What are the main types of jaundice?
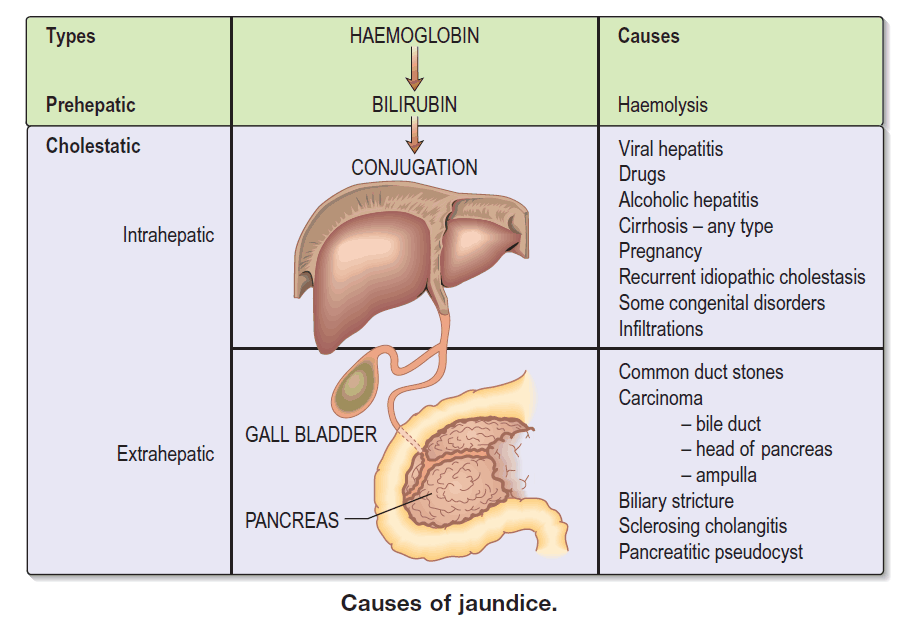
The three main types are prehepatic (hemolytic), hepatic (hepatocellular), and posthepatic (obstructive or cholestatic) jaundice.
What causes prehepatic jaundice?
Prehepatic jaundice is caused by excessive breakdown of red blood cells, leading to unconjugated hyperbilirubinemia, commonly due to hemolytic anemia.
What causes hepatic jaundice?
Hepatic jaundice results from liver cell dysfunction due to hepatitis, cirrhosis, drug-induced liver injury, alcohol-related liver disease, or metabolic disorders.
What causes posthepatic or obstructive jaundice?
Posthepatic jaundice is caused by obstruction of bile flow due to gallstones, pancreatic cancer, bile duct strictures, or cholangiocarcinoma.
How can unconjugated and conjugated jaundice be differentiated?
Unconjugated jaundice is usually due to hemolysis or genetic disorders, while conjugated jaundice is associated with bile obstruction or liver excretory dysfunction.
What laboratory tests help in differentiating jaundice causes?
Key tests include total and direct bilirubin, ALT, AST, ALP, GGT, complete blood count, reticulocyte count, viral hepatitis markers, and coagulation profile.
What clinical features suggest obstructive jaundice?
Pale stools, dark urine, severe itching, elevated ALP and GGT, and progressive painless jaundice suggest obstructive jaundice.
What clinical features suggest hemolytic jaundice?
Anemia, splenomegaly, elevated reticulocyte count, unconjugated hyperbilirubinemia, and absence of bilirubin in urine suggest hemolytic jaundice.
What are red flag causes of jaundice?
Red flag causes include acute liver failure, pancreatic cancer, cholangiocarcinoma, biliary atresia in infants, severe drug toxicity, and sepsis.
Why is stool color important in jaundice evaluation?
Pale or clay-colored stools indicate biliary obstruction, while normal-colored stools suggest non-obstructive jaundice.
What imaging studies are useful in jaundice workup?
Ultrasound abdomen is first-line, followed by MRCP, CT scan, or ERCP when obstruction or malignancy is suspected.
What genetic disorders cause jaundice?
Genetic causes include Gilbert syndrome, Crigler–Najjar syndrome, Dubin–Johnson syndrome, Rotor syndrome, Wilson disease, and alpha-1 antitrypsin deficiency.
What causes jaundice in newborns?
Neonatal jaundice may be physiologic or caused by hemolysis, infection, biliary atresia, metabolic disorders, or genetic bilirubin conjugation defects.
How does alcohol cause jaundice?
Alcohol damages hepatocytes, impairs bilirubin metabolism, and causes alcoholic hepatitis or cirrhosis leading to hepatic jaundice.
What role does sepsis play in jaundice?
Sepsis can cause cholestasis due to impaired bile excretion, resulting in conjugated hyperbilirubinemia.
What is painless progressive jaundice a sign of?
Painless progressive jaundice is commonly associated with pancreatic cancer or cholangiocarcinoma.
What is the first step in evaluating a patient with jaundice?
The first step is to determine whether hyperbilirubinemia is conjugated or unconjugated and assess liver enzyme patterns.
What liver enzyme pattern suggests cholestatic jaundice?
Marked elevation of ALP and GGT compared to ALT and AST suggests cholestatic or obstructive jaundice.
Why is jaundice considered a serious clinical sign?
Jaundice can indicate life-threatening conditions such as acute liver failure, malignancy, severe infection, or major biliary obstruction, requiring urgent evaluation.
MCQ Test - Differential Diagnosis of Jaundice Complete Causes Types Clinical Approach
Progress:
0/15
Time: 00:00
Test Results
0%
0/15
0
Correct Answers
0
Wrong Answers
00:00
Time Taken
0
Skipped