Medical Disclaimer: This is educational content only, not medical advice. Consult a licensed healthcare provider for diagnosis/treatment. Information based on sources like WHO/CDC guidelines (last reviewed: 2026-02-13).
This article is being expanded for more depth. Check back soon!
Edema Causes Symptoms Diagnosis and Complete Medical Management
Frequently Asked Questions
What is edema?
Edema is the abnormal accumulation of fluid in the interstitial tissues, leading to visible or palpable swelling of body parts.
What are the main mechanisms causing edema?
Edema is caused by increased capillary hydrostatic pressure, decreased plasma oncotic pressure, increased capillary permeability, lymphatic obstruction, and renal sodium and water retention.
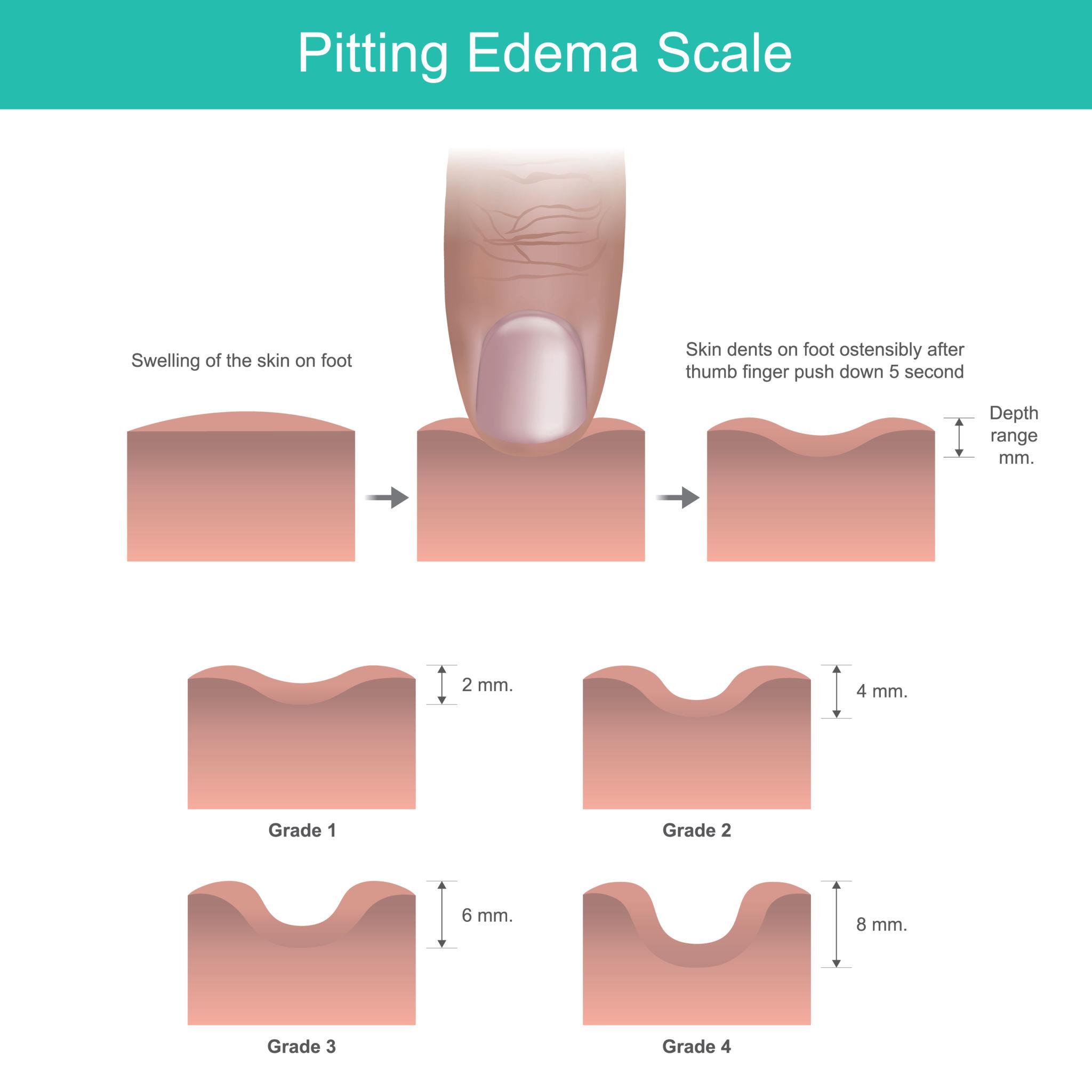
What is the difference between pitting and non-pitting edema?
Pitting edema leaves a persistent indentation when pressure is applied and is seen in cardiac, renal, and hepatic causes, while non-pitting edema does not pit and occurs in lymphedema and myxedema.
Why does nephrotic syndrome cause edema?
Nephrotic syndrome causes massive protein loss in urine leading to hypoalbuminemia, reduced plasma oncotic pressure, and fluid shift into interstitial spaces.
Why is edema worse in the evening in heart failure?
In heart failure, prolonged standing increases venous pressure in dependent areas, leading to fluid accumulation that worsens by evening.
What causes non-pitting edema in hypothyroidism?
Deposition of glycosaminoglycans in the interstitial tissue leads to water retention, resulting in non-pitting edema called myxedema.
What is anasarca?
Anasarca refers to severe, generalized edema involving the entire body, often seen in advanced heart failure, nephrotic syndrome, or liver cirrhosis.
Which drugs commonly cause edema?
Common drugs causing edema include calcium channel blockers, NSAIDs, corticosteroids, and thiazolidinediones.
How is edema evaluated clinically?
Clinical evaluation includes assessing pitting, distribution, timing of swelling, associated symptoms, and systemic signs such as raised JVP, proteinuria, or ascites.
What is the general approach to managing edema?
Management includes treating the underlying cause, salt and fluid restriction, limb elevation, compression therapy when appropriate, and diuretics when indicated.
MCQ Test - Edema Causes Symptoms Diagnosis and Complete Medical Management
Progress:
0/45
Time: 00:00
Test Results
0%
0/45
0
Correct Answers
0
Wrong Answers
00:00
Time Taken
0
Skipped