Medical Disclaimer: This is educational content only, not medical advice. Consult a licensed healthcare provider for diagnosis/treatment. Information based on sources like WHO/CDC guidelines (last reviewed: 2026-02-13).
Metabolic Syndrome X Causes Diagnosis Management and Prevention Guide
Frequently Asked Questions
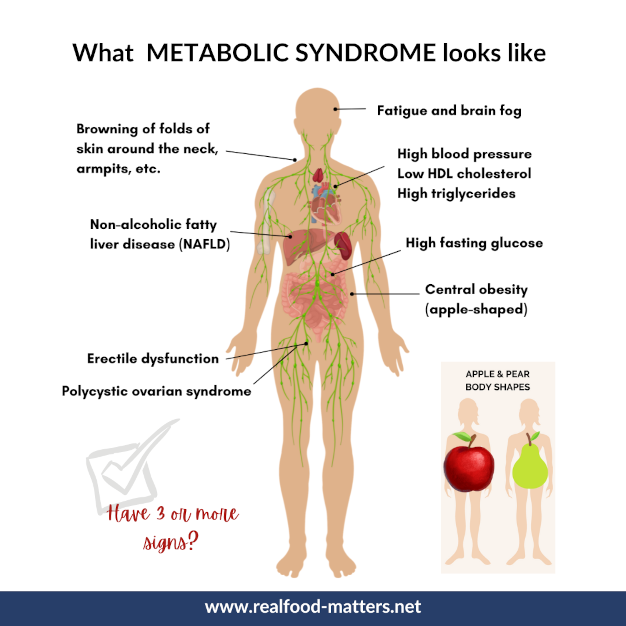
What is metabolic syndrome X?
Metabolic syndrome X is a cluster of metabolic abnormalities including central obesity, insulin resistance, dyslipidemia, hypertension, and impaired glucose metabolism that together increase the risk of type 2 diabetes and cardiovascular disease.
What causes metabolic syndrome?
The primary cause is insulin resistance, often driven by central (visceral) obesity, physical inactivity, genetic predisposition, unhealthy diet, and chronic low-grade inflammation.
How is metabolic syndrome diagnosed?
It is diagnosed using criteria such as NCEP ATP III or IDF. Diagnosis usually requires the presence of at least three abnormalities among waist circumference, blood pressure, fasting glucose, triglycerides, and HDL cholesterol.
Why is central obesity important in metabolic syndrome?
Central obesity reflects excess visceral fat, which releases inflammatory cytokines and free fatty acids that worsen insulin resistance and accelerate atherosclerosis.
What are the main health risks of metabolic syndrome?
Major risks include type 2 diabetes mellitus, coronary artery disease, stroke, nonalcoholic fatty liver disease, chronic kidney disease, and increased all-cause mortality.
Can metabolic syndrome occur with normal body weight?
Yes. Some individuals, especially South Asians, may develop metabolic syndrome despite normal BMI due to excess visceral fat and genetic susceptibility.
What lifestyle changes are most effective in treating metabolic syndrome?
Weight reduction of 5–10%, regular aerobic and resistance exercise, a Mediterranean-style diet, smoking cessation, reduced alcohol intake, adequate sleep, and stress management are most effective.
Is medication always required for metabolic syndrome?
Not always. Lifestyle modification is first-line therapy. Medications are used to treat individual components such as hypertension, dyslipidemia, or hyperglycemia when lifestyle measures are insufficient.
Which drugs are commonly used in metabolic syndrome?
Commonly used drugs include metformin for insulin resistance, statins for dyslipidemia, ACE inhibitors or ARBs for hypertension, and fibrates for severe hypertriglyceridemia.
Does metabolic syndrome always lead to diabetes?
No, but it significantly increases the risk. Early identification and aggressive lifestyle intervention can delay or prevent progression to type 2 diabetes.
Is metabolic syndrome reversible?
Yes. With sustained weight loss, dietary changes, physical activity, and risk-factor control, many features of metabolic syndrome can improve or resolve.
How does metabolic syndrome increase cardiovascular risk?
It promotes endothelial dysfunction, inflammation, atherogenic dyslipidemia, and hypertension, leading to accelerated atherosclerosis and higher rates of heart attack and stroke.
What role does diet play in metabolic syndrome management?
Diet is central. Diets rich in whole grains, fruits, vegetables, lean proteins, healthy fats, and low in refined carbohydrates and trans fats improve insulin sensitivity and lipid profiles.
Should patients with metabolic syndrome take aspirin?
Aspirin is not routinely recommended for primary prevention and should be considered only after individualized cardiovascular and bleeding risk assessment.
How often should patients with metabolic syndrome be monitored?
Regular follow-up every 3–12 months is recommended to monitor weight, waist circumference, blood pressure, glucose levels, lipid profile, and overall cardiovascular risk.
MCQ Test - Metabolic Syndrome X Causes Diagnosis Management and Prevention Guide
Progress:
0/15
Time: 00:00
Test Results
0%
0/15
0
Correct Answers
0
Wrong Answers
00:00
Time Taken
0
Skipped