Medical Disclaimer: This is educational content only, not medical advice. Consult a licensed healthcare provider for diagnosis/treatment. Information based on sources like WHO/CDC guidelines (last reviewed: 2026-02-13).
This article is being expanded for more depth. Check back soon!
Bundle Branch Block Clinical Features Diagnosis and Management Guide
Frequently Asked Questions
What is a bundle branch block?
A bundle branch block is a cardiac conduction abnormality in which electrical impulses are delayed or blocked in the right or left bundle branch of the His–Purkinje system, resulting in widened QRS complexes and asynchronous ventricular depolarization on ECG.
What is the difference between right and left bundle branch block?
Right bundle branch block affects right ventricular depolarization and is often benign, while left bundle branch block affects left ventricular depolarization and is usually associated with underlying structural heart disease and worse prognosis.
What are the common causes of left bundle branch block?
Common causes include hypertension with left ventricular hypertrophy, ischemic heart disease, cardiomyopathy, aortic stenosis, myocardial infarction, and degenerative conduction system disease.
Is bundle branch block always symptomatic?
No, many patients with bundle branch block are asymptomatic. Symptoms such as syncope, dizziness, or dyspnea usually indicate associated heart disease or progression to advanced conduction block.
Why is new-onset left bundle branch block with chest pain considered dangerous?
New-onset left bundle branch block can mask ischemic ECG changes and is treated as a STEMI equivalent because it often represents acute myocardial infarction requiring urgent reperfusion.
How is bundle branch block diagnosed?
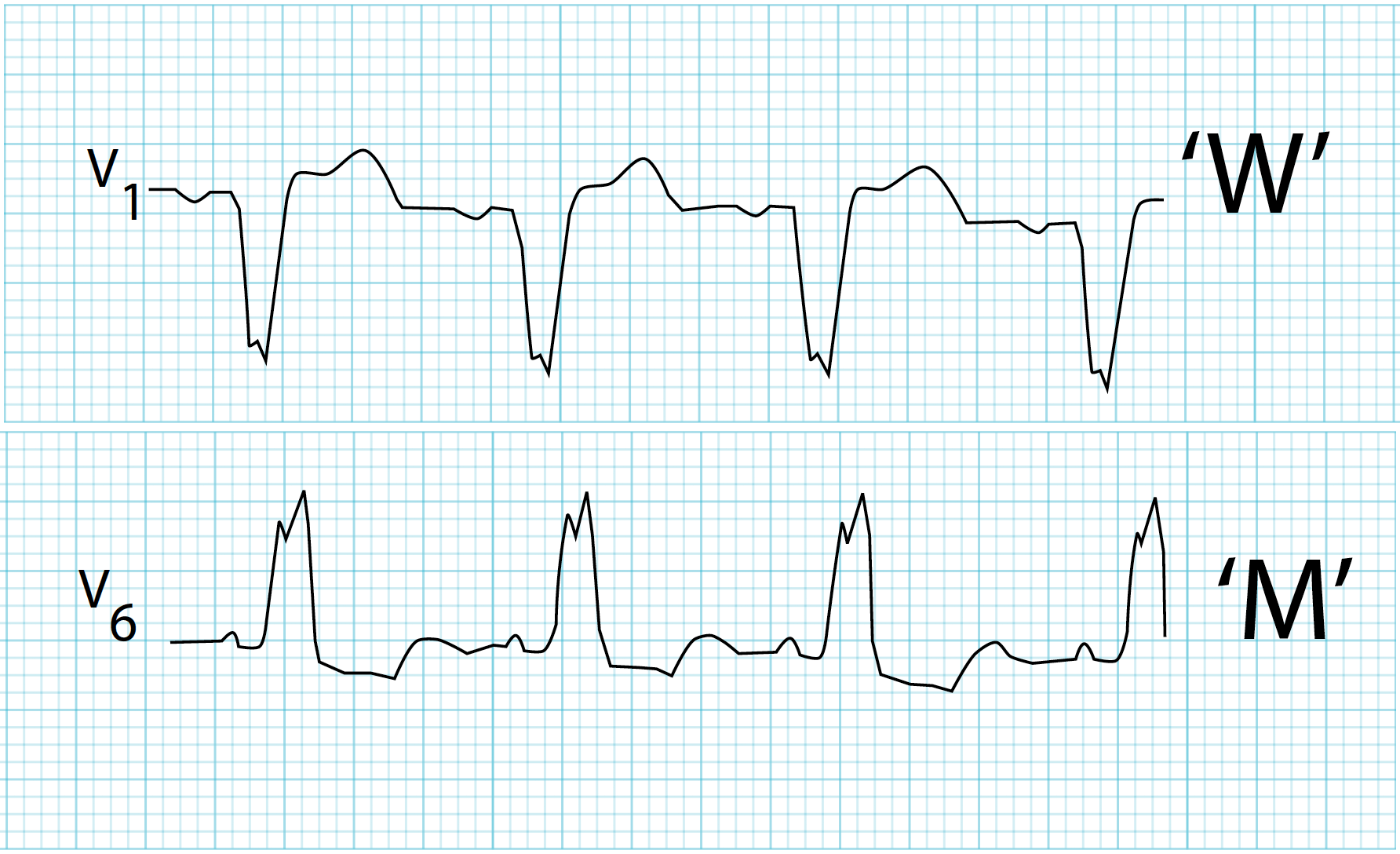
Diagnosis is made using a 12-lead ECG showing QRS duration of 120 ms or more with characteristic morphologic patterns specific to right or left bundle branch block.
Does right bundle branch block require treatment?
Isolated asymptomatic right bundle branch block usually does not require treatment. Management focuses on identifying and treating any underlying cardiac or pulmonary condition.
When is a pacemaker indicated in bundle branch block?
A pacemaker is indicated in patients with bundle branch block who develop symptomatic high-grade atrioventricular block, recurrent syncope due to conduction disease, alternating bundle branch block, or trifascicular disease.
What is the role of cardiac resynchronization therapy in bundle branch block?
Cardiac resynchronization therapy is recommended in patients with heart failure, reduced ejection fraction (≤35%), left bundle branch block morphology, and wide QRS duration to improve symptoms and survival.
What is the prognosis of bundle branch block?
Prognosis depends on the type and underlying cause. Isolated right bundle branch block has a good prognosis, while left bundle branch block is associated with increased risk of heart failure, arrhythmias, and cardiovascular mortality.
MCQ Test - Bundle Branch Block Clinical Features Diagnosis and Management Guide
Progress:
0/15
Time: 00:00
Test Results
0%
0/15
0
Correct Answers
0
Wrong Answers
00:00
Time Taken
0
Skipped