Medical Disclaimer: This is educational content only, not medical advice. Consult a licensed healthcare provider for diagnosis/treatment. Information based on sources like WHO/CDC guidelines (last reviewed: 2026-02-13).
Infective Endocarditis Clinical Features Diagnosis and Management Guide
Frequently Asked Questions
What is infective endocarditis?
Infective endocarditis is a microbial infection of the endocardial surface of the heart, most commonly involving the heart valves, characterized by vegetation formation, systemic embolization, and immune-mediated complications.
Which organisms most commonly cause infective endocarditis?
The most common organisms are Staphylococcus aureus, viridans streptococci, Enterococci, coagulase-negative staphylococci (especially in prosthetic valves), and HACEK organisms.
What are the major risk factors for infective endocarditis?
Major risk factors include prosthetic heart valves, previous infective endocarditis, congenital heart disease, rheumatic or degenerative valve disease, intravenous drug use, indwelling catheters, and immunosuppression.
What are the classic clinical features of infective endocarditis?
Common features include fever, new or changing heart murmur, embolic phenomena, vascular signs such as Janeway lesions, immunologic signs such as Osler nodes and glomerulonephritis, and systemic manifestations like weight loss and fatigue.
What are Janeway lesions and Osler nodes?
Janeway lesions are painless erythematous lesions on palms and soles caused by septic emboli, while Osler nodes are painful nodules on fingers or toes due to immune complex deposition.
What investigations are essential for diagnosing infective endocarditis?
Essential investigations include multiple blood cultures before antibiotics, echocardiography (TTE followed by TEE if needed), inflammatory markers, urine analysis, and imaging for embolic complications.
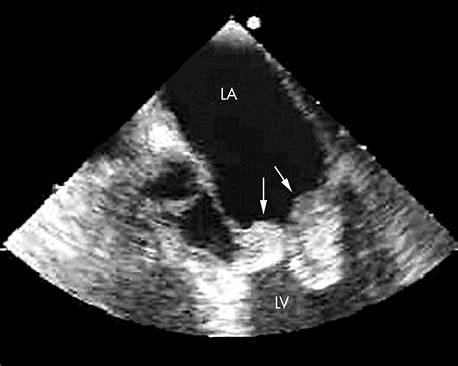
Why is transesophageal echocardiography preferred in many cases?
TEE has higher sensitivity than transthoracic echocardiography, especially for detecting vegetations on prosthetic valves, periannular abscesses, and small lesions.
What are the Duke criteria used for?
The modified Duke criteria are used to establish the diagnosis of infective endocarditis based on a combination of clinical, microbiological, and echocardiographic findings.
What is culture-negative infective endocarditis?
Culture-negative infective endocarditis refers to cases where blood cultures are negative, commonly due to prior antibiotic use or infection with fastidious organisms such as Coxiella burnetii or Bartonella species.
How long is antibiotic therapy usually required?
Intravenous antibiotic therapy is typically required for 4 to 6 weeks for native valve endocarditis and at least 6 weeks for prosthetic valve endocarditis.
Why is combination antibiotic therapy used in some cases?
Combination therapy is used to achieve bactericidal synergy, particularly in enterococcal endocarditis and prosthetic valve infections.
What are the indications for surgical management in infective endocarditis?
Indications include acute heart failure due to valve dysfunction, uncontrolled infection, periannular abscess, recurrent embolization, large vegetations, and prosthetic valve dehiscence.
What are the most common complications of infective endocarditis?
Complications include heart failure, stroke, systemic embolization, renal failure, conduction abnormalities, mycotic aneurysms, and death.
Why are intravenous drug users prone to right-sided infective endocarditis?
Injection of contaminated material introduces bacteria directly into the venous circulation, commonly infecting the tricuspid valve.
What is the role of antibiotic prophylaxis in infective endocarditis?
Antibiotic prophylaxis is recommended only for high-risk patients undergoing certain dental procedures to prevent bacteremia-induced endocarditis.
MCQ Test - Infective Endocarditis Clinical Features Diagnosis and Management Guide
Progress:
0/20
Time: 00:00
Test Results
0%
0/20
0
Correct Answers
0
Wrong Answers
00:00
Time Taken
0
Skipped