Medical Disclaimer: This is educational content only, not medical advice. Consult a licensed healthcare provider for diagnosis/treatment. Information based on sources like WHO/CDC guidelines (last reviewed: 2026-02-13).
Ischemic Heart Disease Comprehensive Clinical Guide Diagnosis Management and Prevention
Frequently Asked Questions
What is ischemic heart disease?
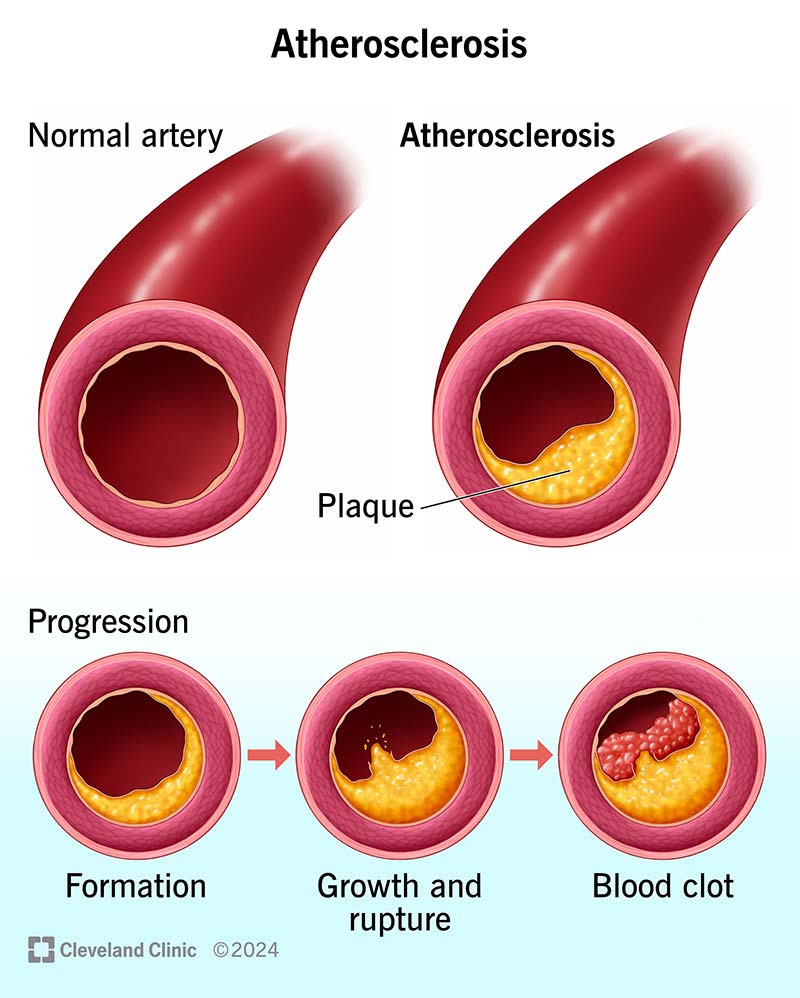
Ischemic heart disease is a condition caused by reduced blood supply to the heart muscle due to narrowing or blockage of coronary arteries, most commonly from atherosclerosis.
What are the main causes of ischemic heart disease?
The main causes include coronary atherosclerosis, plaque rupture with thrombosis, coronary artery spasm, and microvascular dysfunction. Risk factors include smoking, diabetes, hypertension, dyslipidemia, and obesity.
What are the common symptoms of ischemic heart disease?
Typical symptoms include chest pain or pressure, exertional angina, shortness of breath, fatigue, diaphoresis, and in some cases silent ischemia especially in diabetics and elderly patients.
What is the difference between stable angina and unstable angina?
Stable angina occurs predictably with exertion and is relieved by rest or nitrates, while unstable angina occurs at rest or with minimal exertion and indicates a high risk of myocardial infarction.
What investigations are used to diagnose ischemic heart disease?
Diagnosis includes ECG, cardiac biomarkers (troponin), stress testing, echocardiography, coronary CT angiography, and invasive coronary angiography when indicated.
What is acute coronary syndrome?
Acute coronary syndrome refers to a spectrum of conditions caused by acute myocardial ischemia, including unstable angina, NSTEMI, and STEMI.
How is STEMI different from NSTEMI?
STEMI shows ST-segment elevation on ECG due to complete coronary occlusion, while NSTEMI shows ischemic ECG changes without ST elevation and partial coronary occlusion.
What is the first-line treatment in suspected acute coronary syndrome?
Immediate treatment includes aspirin, ECG monitoring, cardiac biomarkers, anti-ischemic therapy, and rapid assessment for reperfusion strategy.
What is the preferred reperfusion strategy for STEMI?
Primary percutaneous coronary intervention is preferred if it can be performed within guideline-recommended time; otherwise fibrinolytic therapy is used when PCI is not promptly available.
What medications are commonly used in ischemic heart disease?
Common medications include antiplatelets (aspirin, P2Y12 inhibitors), statins, beta-blockers, ACE inhibitors or ARBs, nitrates, and anticoagulants in selected cases.
What is dual antiplatelet therapy?
Dual antiplatelet therapy consists of aspirin plus a P2Y12 inhibitor and is used after ACS or PCI to prevent stent thrombosis and recurrent ischemic events.
How long should dual antiplatelet therapy be continued after ACS?
In most ACS patients, dual antiplatelet therapy is recommended for at least 12 months unless there is a high bleeding risk.
What is the role of statins in ischemic heart disease?
Statins reduce LDL cholesterol, stabilize atherosclerotic plaques, reduce inflammation, and significantly lower the risk of future cardiovascular events.
When is coronary artery bypass grafting preferred over PCI?
CABG is preferred in patients with left main disease, triple-vessel disease especially in diabetics, and in those with reduced left ventricular function.
What are common complications of ischemic heart disease?
Complications include heart failure, arrhythmias, mechanical complications like papillary muscle rupture, ventricular septal rupture, sudden cardiac death, and ischemic cardiomyopathy.
What is ischemic cardiomyopathy?
Ischemic cardiomyopathy is chronic left ventricular dysfunction resulting from repeated or extensive myocardial ischemia or infarction.
What lifestyle changes help prevent ischemic heart disease?
Smoking cessation, regular physical activity, heart-healthy diet, weight control, blood pressure control, diabetes management, and stress reduction are essential.
Can ischemic heart disease be silent?
Yes, especially in diabetics and elderly patients, ischemia may occur without chest pain and is known as silent ischemia.
What is the prognosis of ischemic heart disease?
Prognosis depends on extent of coronary disease, left ventricular function, timely reperfusion, adherence to medical therapy, and lifestyle modification.
How does cardiac rehabilitation benefit patients with ischemic heart disease?
Cardiac rehabilitation improves exercise tolerance, reduces mortality, enhances quality of life, and promotes long-term adherence to lifestyle and medical therapy.
MCQ Test - Ischemic Heart Disease Comprehensive Clinical Guide Diagnosis Management and Prevention
Progress:
0/15
Time: 00:00
Test Results
0%
0/15
0
Correct Answers
0
Wrong Answers
00:00
Time Taken
0
Skipped