Medical Disclaimer: This is educational content only, not medical advice. Consult a licensed healthcare provider for diagnosis/treatment. Information based on sources like WHO/CDC guidelines (last reviewed: 2026-02-13).
This article is being expanded for more depth. Check back soon!
Congestive Heart Failure Comprehensive Guide Diagnosis Classification and Management
Frequently Asked Questions
What is congestive heart failure?
Congestive heart failure is a clinical syndrome in which the heart is unable to pump sufficient blood to meet the metabolic demands of the body or can do so only at elevated filling pressures, leading to pulmonary and or systemic congestion.
What are the main types of congestive heart failure?
The main types are heart failure with reduced ejection fraction (HFrEF), heart failure with preserved ejection fraction (HFpEF), and heart failure with mildly reduced ejection fraction (HFmrEF).
What are the most common causes of congestive heart failure?
Common causes include ischemic heart disease, long standing hypertension, valvular heart disease, cardiomyopathies, arrhythmias, and congenital heart disease.
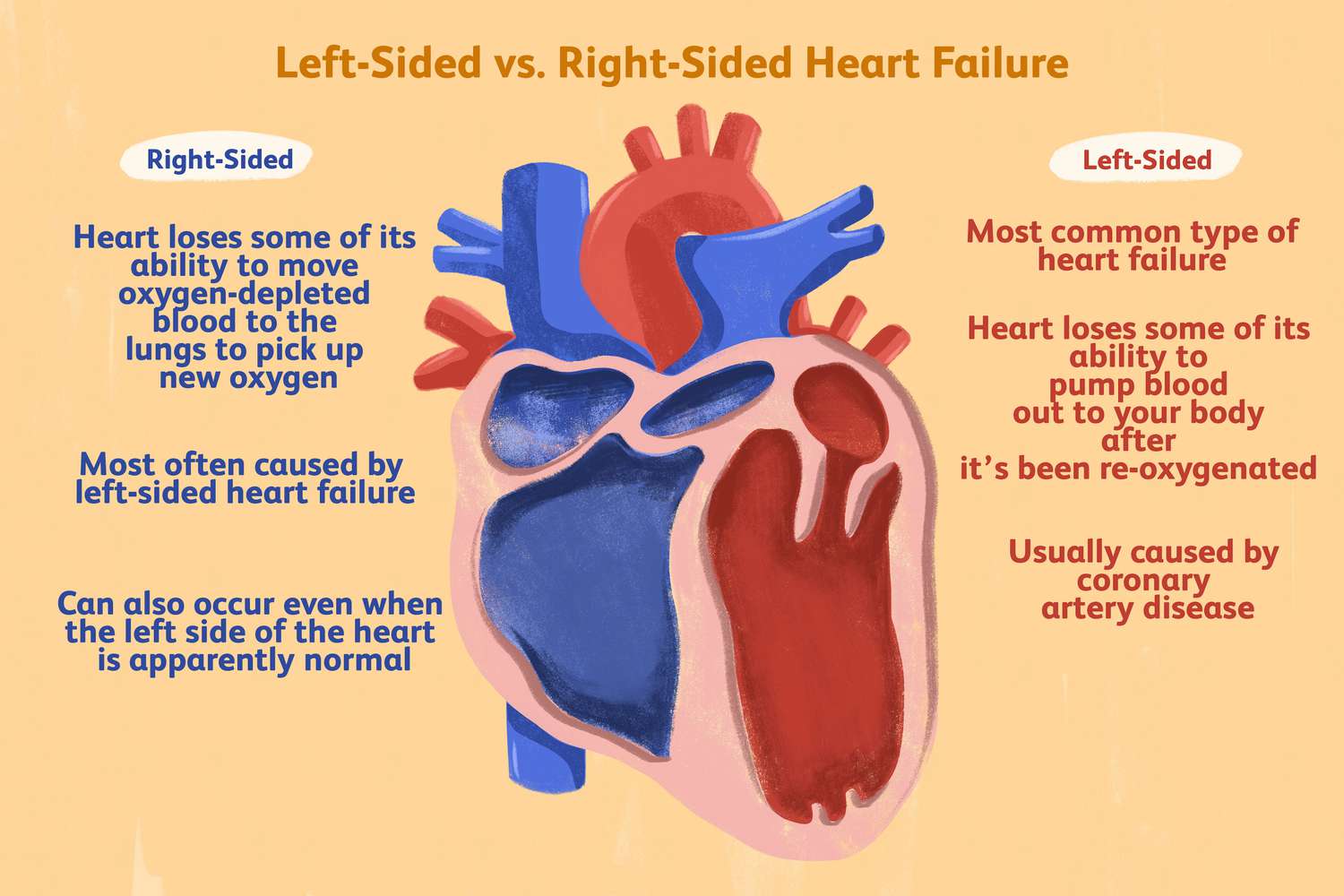
What symptoms suggest left sided heart failure?
Left sided heart failure commonly presents with dyspnea on exertion, orthopnea, paroxysmal nocturnal dyspnea, cough, and pulmonary edema.
What symptoms indicate right sided heart failure?
Right sided heart failure presents with raised jugular venous pressure, hepatomegaly, ascites, peripheral edema, and abdominal discomfort.
What investigations are essential for diagnosing heart failure?
Key investigations include echocardiography to assess ejection fraction, BNP or NT-proBNP levels, ECG, chest X-ray, renal function tests, electrolytes, and complete blood count.
What is the role of BNP in heart failure diagnosis?
BNP and NT-proBNP are markers of myocardial stretch; normal levels make heart failure unlikely, while elevated levels support the diagnosis and help assess severity.
What is guideline directed medical therapy for HFrEF?
Guideline directed medical therapy includes ACE inhibitors or ARNI, evidence based beta blockers, mineralocorticoid receptor antagonists, SGLT2 inhibitors, and diuretics for symptom control.
Do diuretics reduce mortality in heart failure?
Diuretics provide symptomatic relief by reducing congestion but do not independently reduce mortality in heart failure.
Why are beta blockers important in heart failure?
Beta blockers reduce sympathetic overactivity, prevent arrhythmias, reverse remodeling, and significantly reduce mortality and hospitalization in HFrEF.
What is acute decompensated heart failure?
Acute decompensated heart failure is a sudden worsening of chronic or new onset heart failure characterized by pulmonary edema, volume overload, or low cardiac output.
What precipitating factors commonly cause heart failure decompensation?
Common precipitants include infection, myocardial infarction, uncontrolled hypertension, arrhythmias, renal failure, excess salt intake, and non compliance with medications.
How is HFpEF managed?
Management of HFpEF focuses on blood pressure control, diuretics for congestion, treatment of atrial fibrillation, and management of comorbidities such as diabetes and obesity.
When is an implantable cardioverter defibrillator indicated in heart failure?
An ICD is indicated in patients with LVEF 35 percent or less despite optimal medical therapy to prevent sudden cardiac death.
What lifestyle modifications are essential in heart failure management?
Key lifestyle measures include salt restriction, fluid restriction, daily weight monitoring, smoking cessation, limited alcohol intake, regular physical activity, and vaccination.
MCQ Test - Congestive Heart Failure Comprehensive Guide Diagnosis Classification and Management
Progress:
0/15
Time: 00:00
Test Results
0%
0/15
0
Correct Answers
0
Wrong Answers
00:00
Time Taken
0
Skipped