Medical Disclaimer: This is educational content only, not medical advice. Consult a licensed healthcare provider for diagnosis/treatment. Information based on sources like WHO/CDC guidelines (last reviewed: 2026-02-13).
This article is being expanded for more depth. Check back soon!
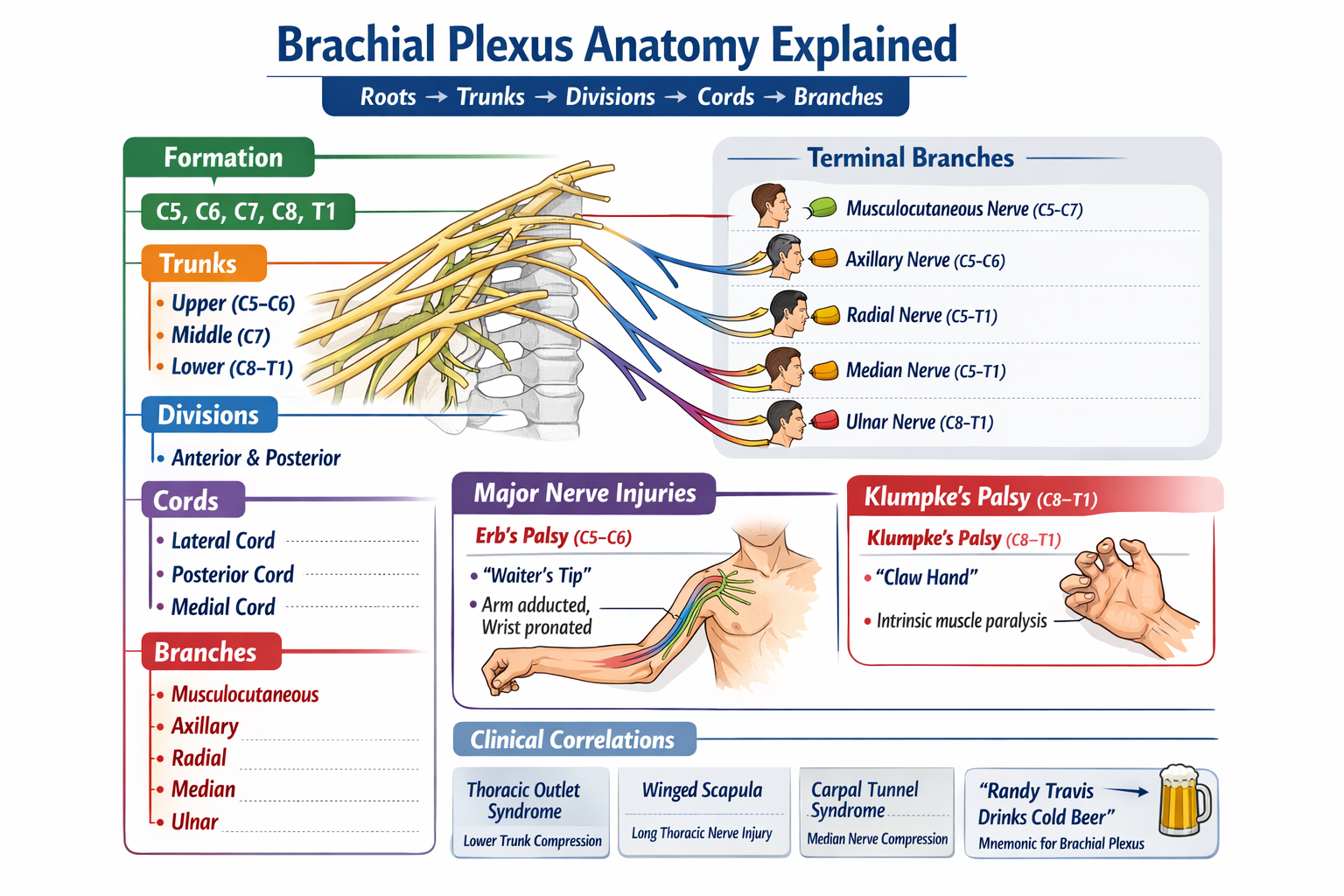
Brachial Plexus Anatomy Explained with Roots Trunks Cords Branches and Clinical Correlations
Frequently Asked Questions
What is the brachial plexus?
The brachial plexus is a network of ventral rami of spinal nerves C5 to T1 that provides motor, sensory, and sympathetic innervation to the upper limb.
Which spinal nerve roots form the brachial plexus?
The brachial plexus is formed by the ventral rami of C5, C6, C7, C8, and T1 spinal nerves.
What is the correct order of components of the brachial plexus?
The correct order is Roots, Trunks, Divisions, Cords, and Branches.
How many trunks are present in the brachial plexus?
There are three trunks: upper trunk (C5–C6), middle trunk (C7), and lower trunk (C8–T1).
What is the functional significance of anterior and posterior divisions?
Anterior divisions supply flexor compartments of the upper limb, while posterior divisions supply extensor compartments.
Why are the cords of the brachial plexus named lateral, medial, and posterior?
They are named according to their position relative to the second part of the axillary artery.
Which nerve is responsible for winged scapula and why?
The long thoracic nerve causes winged scapula when injured because it supplies the serratus anterior muscle.
What is Erb palsy and which nerve roots are involved?
Erb palsy is an upper trunk injury involving C5–C6 nerve roots, resulting in a waiter’s tip deformity.
What is Klumpke palsy and what are its key features?
Klumpke palsy is a lower trunk injury (C8–T1) characterized by intrinsic hand muscle paralysis, claw hand, and sometimes Horner syndrome.
Which nerve arises from all roots of the brachial plexus?
The median nerve receives fibers from all roots C5 to T1.
Which brachial plexus nerve pierces the coracobrachialis muscle?
The musculocutaneous nerve pierces the coracobrachialis muscle.
Which nerve injury causes wrist drop?
Radial nerve injury causes wrist drop due to paralysis of wrist extensors.
What is thoracic outlet syndrome in relation to the brachial plexus?
Thoracic outlet syndrome involves compression of the lower trunk of the brachial plexus as it passes between the clavicle and first rib.
Which cord gives rise to the ulnar nerve?
The ulnar nerve arises from the medial cord of the brachial plexus.
Why is the brachial plexus clinically important?
It is crucial because injuries at different levels produce characteristic motor and sensory deficits, aiding localization of nerve damage.
MCQ Test - Brachial Plexus Anatomy Explained with Roots Trunks Cords Branches and Clinical Correlations
Progress:
0/0
Time: 00:00
No MCQs available for this article.